The diagnosis of Mycoplasma bovis is becoming more and more common on dairy farms, it can cause disease in both calves and adult cattle. It is a notoriously difficult bug to treat, and even then vaccination has historically proved difficult.
We have previously relied onautogenous vaccine (those producedin a lab using M. bovis cultured frominfected animals), however there is now a vaccine available in North America that we have been able to import using a SIC. A recent report of a vet led study has looked at growth rates, mortality and antimicrobial usage in 1582 calves born into eight herds in Scotland. Cows and in-calf heifers were vaccinated at drying off or at least 4 weeks pre-calving. Calves then received a booster at 60d old, in line with the US protocol.
Weaned calf mortality fell from 5.8% pre-vaccination to 0.5% postvaccination, whereas in the control farms this remained between 7.3- 7.8%. Antibiotic usage dropped from an average 116.9 PCU/100kg live weight pre-vaccination to 41.45 PCU/100kg post-vaccination, whereas in the control farms, this was seen as an increase in antibiotic usage.
So what is Mycoplasma Bovis?
They are small bacteria distinguished by their lack of cell wall. They are generally, host-specific and there have been 13 species identified in cattle, although not all are implicated in disease. M. Bovis produces a biofilm, changing surface proteins and can persist on mucosal surfaces, enabling them to evade the host immune response, therefore causing disease.

The organism may be carried asymptomatically and the introduction of subclinical animals into the herd is the primary means that a naïve herd becomes infected. The major route of M. bovis transmission is nose to nose contact and aerosol spread. Other routes of infection include ingestion via contaminated milk (i.e feeding waste milk to calves) or via contaminated milking/feeding equipment.

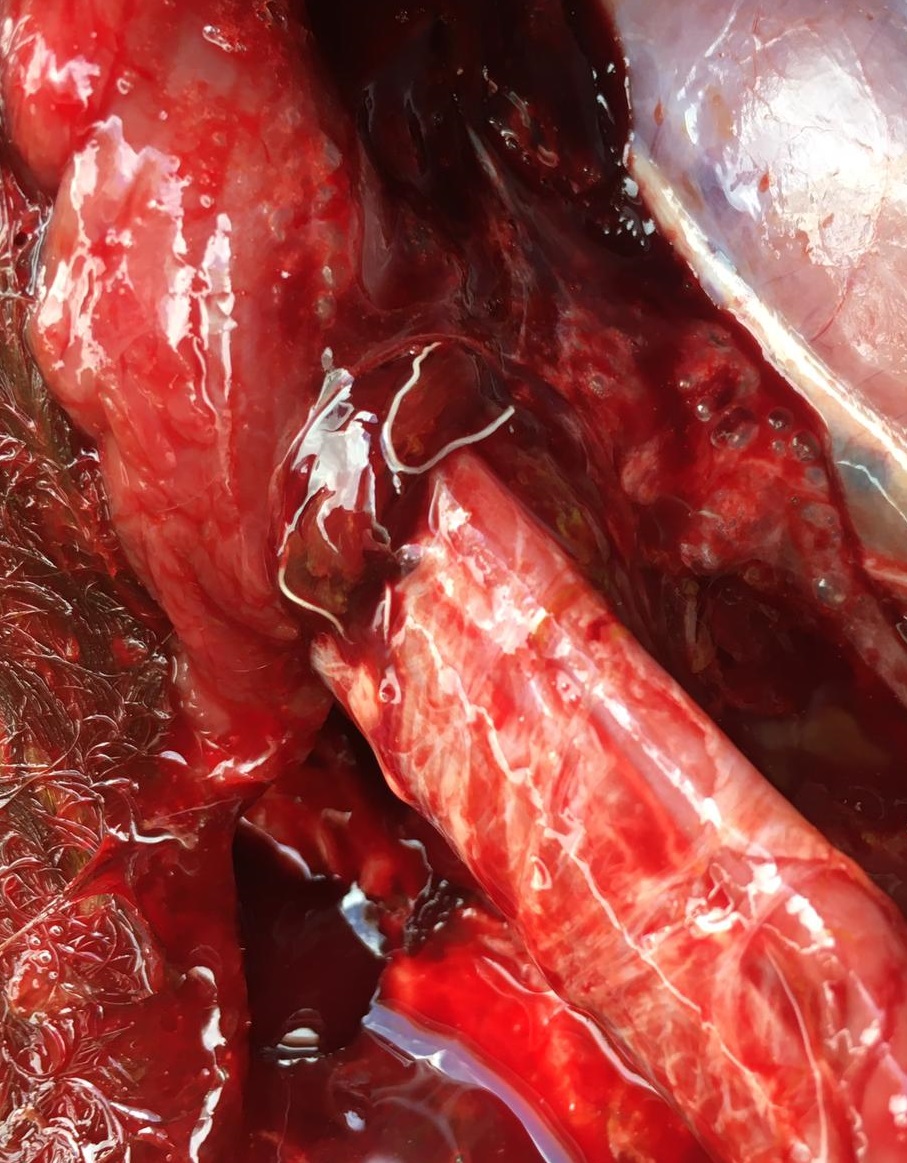
It can also cause pneumonia and can be seen as a key player in the organisms associated with bovine respiratory disease.
Diagnosis of M. Bovis can be difficult due to the low sensitivity and in some cases specificity of the available tests, which can often be complicated by the presence of subclinical infection and intermittent shedding. For clinical cases we can use culture, however, PCR is the detection method of choice.
It proves difficult to treat, its lack of cell wall results in natural resistance to penicillins and cephalosporins and its folic acid independent metabolism results in resistance to TMPS. Whilst other groups of antibiotics do work, the nature of the pathogen, including the ability to create biofilms can reduce a clinical response to treatment. The key to treatment success is early intervention.
Reducing incidence of Mycoplasma bovis on farm involves strict biosecurity.
Where there is known disease in adult animals, the feeding of waste milk should be avoided at all costs. Milking equipment and milk feeding equipment can aid in the transmission of organisms and therefore disinfection is essential. If feeding whole milk, then this must be pasteurised to reduce the bacterial load of M. bovis. A recent study has looked at the risk of M. bovis transmission to the calf via colostrum. A small number of samples found M. bovis DNA, however the study did not conclude that colostrum posed a high risk during a M. bovis outbreak. Where infection pressure is high within a herd, i.e. during an outbreak, it may be beneficial to pasteurise colostrum to reduce the risk of M. bovis transmission.
Prevention is always better than cure. The news of a successful vaccine trial, provides hope of another management strategy we can now use to aid with control the disease in an outbreak.









Leave A Comment